
- Mail: neuroclinic4u@gmail.com
- Emergency Help: +91 6364 249 996
Epilepsy In Children

SAVING AND NURTURING THE DEVELOPING BRAIN.
Epilepsy is largely treated with medicines successfully however there are subset of patients who are resistant to drugs or the drugs fail to control seizures (Drug refractory). An estimated 10.5 million children worldwide have epilepsy. The annual incidence is reported to be 61 to 124 per 100,000 children in developing countries. Any child affected with seizures is not only an awful experience to the family but also the child is equally prone for an unexpected sudden complication endangering the life. Epilepsy in a child is different from adults in numerous ways. Most importantly it is the developing brain, which faces the arrest in the growth and development due to an on-going seizures. The brain, which is normally bustling with activity in a child, comes to a standstill whenever the seizure spreads. This affects the formation of new connections and the neuronal processing in a significant manner. All the important milestones are achieved and new skills are acquired in the first decade of life. This is lost due to the engagement of brain in seizure activity. Rapid brain maturation during early infancy and childhood is responsible for a complex evolution of clinical seizure, EEG and MRI findings. This complexity makes the assessment of the clinical, electrophysiological, and imaging findings very challenging.
What is drug refractory epilepsy (DRE)?
As per the ILAE guidelines the drug refractory epilepsy is defined as a failure to achieve seizure freedom after an adequate trials of two drugs with an optimal dosage for two years and with good compliance. However for paediatric age, this period of two years is not practical as lot more damages can happen in a developing brain as explained earlier. Hence in children, the failure of either 2 or 3 appropriate AEDs or causing disabling seizure side effects and / or disabling AED side effects need to be considered as drug refractory. In general the incidence is 20% - 30%, which can vary widely based on the cause for epilepsy.
What needs to be done?
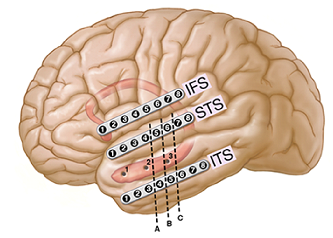
The MR imaging of brain of children is complex in terms of interpretation as the brain is growing and will be immature in terms of myelination. A ‘normal’ MRI report does not rule out small abnormalities and as per the guidelines the MRI has to be repeated at an interval of six months or after two years of age if there is a strong index of suspicion for focal onset seizures. More importantly an experienced team of experts should interpret these complex MRI. Similarly EEG evaluation in infants and young children is extremely difficult because of poorly defined “normal” and “abnormal” EEG patterns of the immature brain. As a result, identifying the location of seizure onset is very difficult, one that needs to be handled with a great deal of expertise. Hence in most paediatric cases would require phase wise evaluation with phase-I involving non-invasive imaging investigations and phase-II involving invasive depth electrode evaluation. Phase-I investigations consist of nuclear medicine with PET (Positron Emission Tomography) scan and SPECT (Single Photon Emission Computed Tomography) scans and MagnetoEncephaloGraphy (MEG). If the phase-I evaluation reveals a focal origin of seizures one can proceed with surgery. If any of these investigations are not helpful in identifying the focus then child needs to be subjected for further investigations with depth electrodes, which are inserted in the brain to record the seizures, which are done with minimal risk.
What are the types of epilepsies in children that can be cured by surgery?
Some of the types of epilepsies, which are drug resistant but cured by surgery are
- Developmental lesions like cortical dysplasia, hamartoma and heterotopia;
- Rasmussen encephalitis,
- Tuberous sclerosis,
- Sturge-Weber syndrome,
- Hemiconvulsion-Hemiplegia-Epilepsy syndrome (HHE),
- Hemimegalencephaly.
- Vascular lesions like AVM, cavernous malformations;
- Injury-related lesions like gliosis (from CVA or trauma);
- With recent advances in imaging, electrophysiology and surgical techniques the infantile spasms, which were largely considered as medical condition hitherto are now recognised as a surgical condition as well.
When to consider surgery for epilepsy?
Surgery is often the treatment option for some of these children with drug refractory epilepsy, not only to control seizures but also to prevent and improve the co-morbid conditions mentioned previously. Young children have a much greater potential for recovery after a surgery, and a significant capacity for reorganization of neurological function. Because many types of paediatric epilepsy syndromes are inherently medically refractory, there is no need to “prove” that drugs are failing before embarking on a surgical course of action. The harmful effects of prolonged seizures and the toxic effects of AEDs on brain development, and cognitive and psychosocial development bolster the argument for early surgery in paediatric epilepsy patients. The RCT trial in paediatric age group to look at the benefits of early surgery confirmed that children and adolescents with drug-resistant epilepsy who had undergone epilepsy surgery had a significantly higher rate of freedom from seizures and better scores with respect to behaviour and quality of life than did those who continued medical therapy alone at 12 months. The potential for significant recovery is highest in the age range of 3–7 years, when the plasticity of the brain peaks. Surgery performed within this time frame may help hasten recovery, and anticipated postoperative impairments may be milder. In well-selected patients, early surgical intervention may prevent the negative cognitive, psychosocial, and developmental effects of seizures.
Hence the goals of surgery in these patients should be
- To prevent the possible harmful consequences of uncontrolled seizures;
- To prevent continued interictal activity resulting in permanent cognitive, behavioural, and psychosocial problems;
- To prevent secondary epileptogenesis; and
- To avoid the adverse effects of AEDs.
What are the surgical options?
Surgery is a well-established modality of treatment in these conditions and the various surgical options can be grouped into those that can render seizure freedom and those, which are palliative.
Hemispherotomy- Though this procedure involves disconnection of the epileptogenic hemisphere from the normal side, the risks involved is lesser that the success rate which is close to 90% which is one of the higher success rates among all the available options. The safety has been enhanced further by the use of minimally invasive options of endoscopic hemispherotomy and hemispherotomy by radiofrequency thermoablation (ROTCH) techniques.
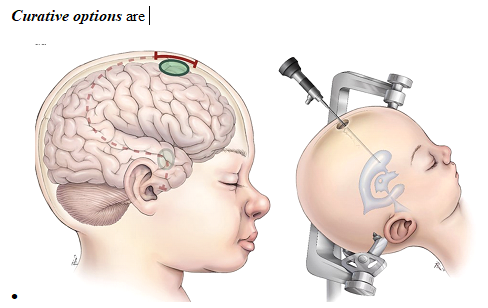
(Electrocorticography) guided lobar resections or disconnective procedures
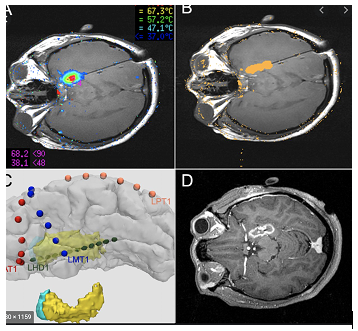
- ⦁ Minimally invasive radiofrequency ablations.
Ecog
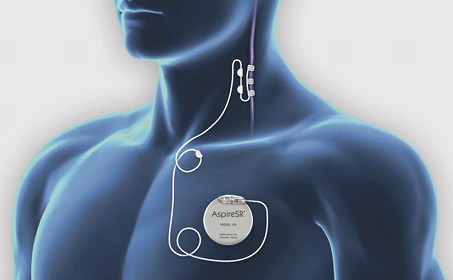
⦁ Palliative options are

However timely recognition of these conditions and referral to specialised centre is an important predictor of the final outcome. Most important concern w.r.t surgery is safety or the risks involved. The advances in the field of Neurosurgery from the introduction of operative microscope onwards the results have been tremendous to an extent that now in India. There are robotic assisted minimally invasive surgeries as well using, which the depth electrodes can be inserted and even the hemispherotomies are performed through tiny twist drill openings. These advances have brought down both the morbidity and mortality. It is a well-known fact that the comprehensive care of children with epilepsy is challenging. Specialised knowledge of and expertise in the medical and surgical management of such patients are required. Thus, a well-coordinated, collaborative relationship between medical and surgical teams in a multidisciplinary environment is critical for successfully managing paediatric epilepsy patients.